



Dedication
This publication is dedicated to the memory of Dr Gina Dillon (1963 - 2017)[1].
Introduction
Despite significant success in control of HIV and delivery of the HPV vaccine, notifications for other sexually transmitted infections (STIs) in Australia continue to increase (Department of Health, 2014). While this increase has been largely across the board, chlamydia and gonorrhea are particular concerns, specifically among younger age cohorts (The Kirby Institute, 2015). Seventy-eight per cent of chlamydia notifications during 2014 were attributed to the 15-29 year old age group (The Kirby Institute, 2015). Given that young adults continue to contribute substantially to Australian STI notification rates, young people under 30 years of age have been included in the Third National Sexually Transmissible Infections Strategy as a priority population, with specific objectives directed towards reducing the incidence of chlamydia and increasing chlamydia testing for this sector of the population (Department of Health, 2014). Young people in Australia, particularly in rural and remote regions, are particularly at risk of STIs as many lack basic comprehensive information about safer sex practices and implications and have limited access to sexual health services (Garrett, Hocking, Chen, Fairley, & Kirkman, 2011; Kang, Skinner, & Usherwood, 2010; Senior, Helmer, Chenhall, & Burbank, 2014).
Within this context, and given exposure to ideas about Health-Promoting Universities (Tsouros, Dowding, Thompson, & Dooris, 1998) and a partnership with Hunter New England Local Health District (HNELHD), the student support staff at a regional university embarked on a process of increasing student awareness of sexual health issues. This focus was specifically chosen due to NSW Health notification data indicating that the Local Government Area (LGA) in which the university is located had the highest chlamydia notification rates in the LHD. There were also anecdotal reports of high chlamydia rates within some residential colleges. Intervention through a number of sexual health promoting activities was undertaken in the university from early 2013. New students on campus were, where possible, provided with talks about sexual health and risk minimisation; free condoms were made available at social events for new students and at cost through vending machines located in some of the residential colleges; posters calling attention to sexual health were placed in key venues across campus from September 2013 to May 2014. At the same time, focus groups with students were conducted to determine how best they would like to access information about sexual health. While the original plan had been to develop peer-driven workshops, evidence from the data collection showed that students most valued anonymity and all-hours access. For these reasons, a sexual health website (http://www.une.edu.au/current-students/support/student-support/counselling/sexual-health) was developed for students which provided information about various aspects of sexual health (STIs; healthy relationships; lesbian, gay, bisexual, transgender, intersex and questioning [LGBTIQ)] sexual health and safer sex practices), as well as links to other reliable sources of sexual health information and services. During the latter half of 2013, HNELHD conducted training with the university health clinic and GPs in the area about managing sexual health problems for young people in order to ensure that health care centres provided young people with appropriate STI screening and treatment.
Methods
A cross-sectional online survey of students was conducted to examine their sexual behaviours and attitudes and to measure exposure to the intervention. A hard-copy of the survey was first piloted on a small sample of (n=8) international students to ensure questions were unambiguous and easily understood. In view of time constraints for further piloting, the survey included, where possible, validated and piloted sexual health knowledge questions drawn from the Australian National Survey of Secondary Students (Smith, Agius, Mitchell, Barrett & Pitt, 2009). The survey also included sexual health attitude questions drawn from a United States national survey (Hoff, Green & Daws, 2003), and questions about sexual behaviour which are standard population health questions. The survey particularly focused on sexual health knowledge about HIV, fertility and cancer because of a belief that more nuanced information about STIs might be missing from this population. No significant change in sexual behaviours pre and post intervention was anticipated in the 18 month period from baseline to endline surveys, however, a positive change in sexual health knowledge and attitudes between baseline and endline data was hypothesised. Differences by exposure to the intervention from baseline and endline data were also assessed.
Study site
This study was conducted with students at a regional university in NSW with a population of approximately 25,000 students. The university has a strong online teaching presence; therefore participants were both students studying online (therefore resident anywhere in Australia or abroad) and those resident in the regional town in which the university was located; either in university colleges or private accommodation. The town has a regional referral hospital and numerous private GPs, including a university health service that offers bulk billing for students. There is no public sexual health clinic in the town and the nearest facility is approximately 90 minutes’ drive away. Recent NSW Health notification data have shown that this LGA has the highest chlamydia rates of its LHD, and might be attributed to the large number of students in the town and limited accessibility to timely sexual health care (Roberts, 2014).
Recruitment of survey participants
In late 2012, an email was sent to all students aged 18-29 years who commenced undergraduate study that year. The email notified students of the survey that asked about their demographics, sexual health knowledge, attitudes and history, as well their current access to sexual health resources, and requested them to complete it anonymously. The online survey included an information page, online consent page, and anonymous responses. This baseline survey was sent to 2,438 students, of whom 452 logged in and made an attempt, and 418 completed the survey. In mid-2014 a second email with a link to an endline or post-intervention survey was sent to all students aged 18-31 years old who had commenced study from 2012; the aim being to capture students in the 2012 sample (some of whom would have turned 31 by then) as well as undergraduate students who had enrolled since that time. The email again notified students of the survey and requested them to complete it anonymously. The endline survey was sent to 5,185 students, of whom 1,016 logged in and made an attempt and 956 completed the survey. Of these 956 students, 105 had also completed the 2012 survey. The low response rate to both the baseline and endline surveys meant than only endline survey data were analysed.
Analysis
Survey data were collected in SurveyMonkey (Palo Alto, Ca, USA, www.surveymonkey.com) and exported to SPSS version 22. Descriptive statistics were compiled for demographic variables and percentage responses for attitude and knowledge questions. Chi-square analyses were conducted to test for significant differences in responses between groups based on gender, relationship status and number of sexual partners. Given that Chi-square contingency table cells involved data from the same sample configured in different ways across different analyses, it was considered appropriate to use a more stringent alpha level; differences were assumed to be significant at the p<0.01 level.
Ethics approval
Ethics approval was granted by the University of New England Human Research Ethics Committee (approval number: H12-173).
Results
Of the 1,016 students who logged into the endline survey and initiated a response, full data were available for 956 students. Responses were heavily weighted towards female students, who comprised almost two-thirds of the participants (Table 1); and reflect the gender profile of new enrolments in the 17 to 29 age group generally (ratio of one male to every two females in 2012 new-student-enrolment-data for this age range). Transgender students accounted for a very small (0.2%) proportion of respondents. The vast majority of participants (96%) identified themselves as non-Indigenous Australians and English speaking. Worth noting is that within the sample, 3.9% identified as Aboriginal, Torres Strait Islander or both (A and/or TSI), which is comparable with 3.3% of students new to this university aged 17 to 29 identifying as A and/or TSI (based on this university’s new-student-enrolment-data for 2012 for this age group). Slightly over half of participating students attended university on campus (57.6%) and the remaining were online students; an over-representation of on-campus students in the survey sample when compared with the 35% who comprised this university’s new-student-enrolment-data in 2012 for the 17 to 29 year old age group. A third of participating students reported living on campus (35.7%). The mean age of participants was 21.9 years. Further demographic information is available in Table 1.
Table 1: Demographic characteristics of student participants (n=956)
.png)
Sexual health behaviours
Of the 956 participants, the majority reported being sexually active in the past 12 months (76.0%). Almost a quarter of participants chose not to answer this question and the remaining 3.9% noted that they had not been sexually active over this time. Focusing on the 728 participants who reported being sexually active in the past 12 months, we asked about health promoting sexual behaviours such as condom use and seeking care or support for sexual health issues.
When asked to report on condom use at last sexual encounter, only 52.5% of participants, shown in Table 2a, reported that they had used condoms at last sex-repeated. The use of condoms at last sex was not associated with the number of sexual partners reported in the last year (p=0.232), however we saw the lowest condom use among those with the highest number of partners in the past 12 months (46.9% of those with 6 or more partners). Condom use, as shown in Table 2b, was associated with relationship status; a significantly lower proportion of participants who were married or in de facto relationships reported using a condom at last sex, compared to those who were single or in a relationship that was not marriage or de facto (p<0.01). Participants reported buying condoms largely from supermarkets, convenience stores and pharmacies (39%). A far smaller proportion got condoms from friends (2.7%) or for free on the university campus (1.8%). Accessing condoms from community or sexual health clinics was rare (0.7%).


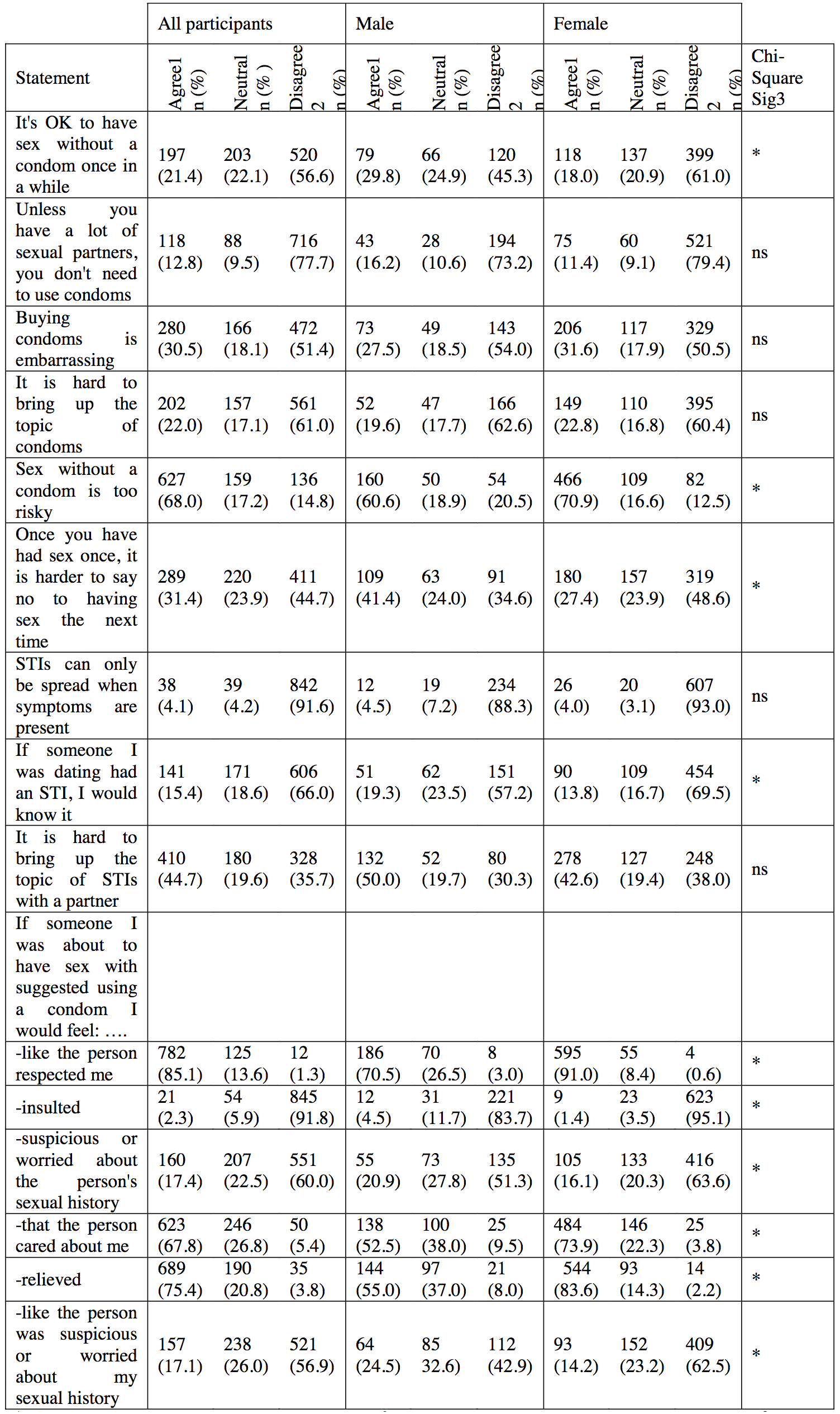
Sexual health attitudes and knowledge
Overall, students who participated in this study had relatively good knowledge about STIs and positive attitudes towards condom use. In a range of questions about knowledge and attitudes (see Table 3); students displayed particularly good knowledge regarding when STI transmission is possible and the need to use condoms irrespective of partner number. Participants were largely positive about condoms, agreeing that if a partner suggested using condoms they would be relieved (75.4% agreed) and feel that their partner respected them (85.1% agreed). Only 2.3% reported that they would feel insulted if a partner suggested condoms, although almost half thought it might make them feel that their partner was suspicious or worried about their sexual history. There were a number of significant (p<0.01) differences by gender: women were significantly more likely to report positive attitudes towards a partner suggesting condom use than were male participants. Despite these largely positive attitudes, more than a third of participants agreed with or felt neutral about the statement ‘If someone I was dating had an STI, I would know it’ and a significant proportion acknowledged the challenges associated with discussing STIs and discussing or obtaining condoms. Almost half (44.7%) thought it was hard to bring up discussion of STIs with a partner and 30.5% said that buying condoms was embarrassing. There were no significant differences by gender for these variables.
.jpg)
Sexual health care: STI screening
Over 80% of sexually active participants had been to a GP or health clinic in the past 12 months however, only 58.8% reported discussing sexual health issues with a health practitioner during this time. Women were significantly more likely to report discussing sexual health issues with a GP in the past 12 months than men (80.8% vs 37.9%; p<0.001). Among sexually active participants, a third had tested for STIs in the previous 12 months. Given that chlamydia is the most prevalent STI in Australia, and particularly among this age group (The Kirby Institute, 2015), we specifically asked about chlamydia testing. A third of sexually active participants had tested for chlamydia in the past 12 months. Women were significantly more likely than men to have tested (39.5% vs 24.1%; p<0.01 for any STI testing; 33.8% compared to 21.5%; p<0.01 for chlamydia testing). Relationship status and number of sexual partners were significantly associated with both STI testing generally and chlamydia testing specifically. Individuals with one to two sexual partners in the past 12 months were less likely to test for any STIs or chlamydia than those with three to five or six or more partners (see Table 4). Married participants were least likely to have tested for STIs in the past 12 months, while those in de facto relationships were most likely to have tested (Table 4).
Among participants who were sexually active in the past 12 months, the most common rationale for STI testing was that this was something that they did ‘routinely’ (14.7%). Other reasons cited were having unprotected sex (8.0%) and a change in relationship status (8.1%). Very few participants said that they had been tested for STIs because of symptoms or because they had sex with someone who had an STI (<5% in both instances). Most participants reporting STI testing had been tested at their GP as opposed to specialised sexual health venues. Participants appeared to be positively inclined to have more regular STI screening. When asked what might prompt them to test for STIs more frequently (more than one response possible), a third noted that they would test if their medical provider offered them a test at their next visit, two-thirds would be more likely to test if the associated visit was bulk billed or free and half felt they would be more likely to test if they received an annual reminder. With regard to an annual reminder for STI testing, more than half would want to receive the reminder via email and just under forty per cent would prefer to receive a text message to their mobile phone.

Exposure to sexual health interventions on campus
Awareness of the three key elements (posters, website, condom-vending machines) of the university sexual health intervention was low. Twenty-eight per cent of participants were not aware of any of the interventions; 37% were aware of only one element of the intervention and only 1.4% were aware of all three. We found that participation was also low. Only 2.7% of all participants had visited the university’s sexual health website. Among students on campus (n=551), 4.3% had purchased condoms from the campus vending machines and 56.9% participants reported that they had seen the posters. Not surprisingly, awareness of the campaign was generally higher among students who lived and studied on campus, compared to all students (on-campus and on-line) combined.
Sexual knowledge and behaviour by intervention exposure
We were interested in examining knowledge about STIs in this population, but focused our attention on three key issues: increased risk of HIV when infected with an STI, problems with fertility associated with STIs and vulnerability to some cancers as a result of STIs. We found that overall knowledge about increased risk of both HIV and cancer was low in this population, although understanding the link between STIs and fertility issues was almost universal. There were no differences in knowledge between those exposed to the university sexual health program (i.e. those who reported awareness of posters, website, condom vending machines) and those not exposed, except for understanding the increased risk of HIV infection associated with having an STI (59.5% vs 49.2%; p=0.016). There were also no differences in sexual health behaviours, such as reporting STI testing, whether they had been exposed to the intervention or not.
Discussion
Overall, students included in this assessment of knowledge and attitudes towards STIs and sexual health had good levels of sexual health knowledge and positive attitudes. However, while condom use was high in single participants and those in non-married or de facto relationships, it was still far from the consistent condom use required for adequate protection against STI transmission.
We found the lowest condom use in the past 12 months was among those potentially at greatest risk of STIs - those reporting more than six sexual partners in the past 12 months, although the highest reports of condom use at last sex was among single participants. This contradictory finding could be related to the small sample size in the study. In contrast to other Australian studies with (male) university students (Flood, 2003), it would appear from these data that while students have positive attitudes towards condoms and are willing to use them, they lack self-efficacy when it comes to taking the initiative in condom use. A third of students thought that buying condoms was embarrassing, and another 20% were neutral about this issue. While the vast majority of participants viewed having condom use suggested by a partner as positive, the fact that two-thirds would feel relieved suggests limited confidence in their own ability to raise this issue and a desire for the decision to be taken out of their hands. Gender differences in attitudes towards a partner suggesting condom use were particularly striking, with women more likely than men to value a partner’s suggestion to use condoms. This finding is not surprising and in keeping with social constructions of the difference between male and female sexual agency, acceptability of perceived sexual availability and concerns with pregnancy. Other research with Australian university students has found that different factors affect condom use with regular and casual partners. Specifically, condom use in casual sexual relationships tends to be determined by interaction between the partners during the sexual encounter. With casual partners, condom use is likely to be determined by the partner’s intention to use condoms rather than one’s own intentions (de Visser & Smith, 2001). Our findings appear to echo this previous study.
Participants in this sample had significantly higher STI testing rates than has previously been documented among Australians in this age group. (Kong et al., 2011) reported testing rates over 12 months adjusted for the proportion of the population sexually active of 12.1% for women and 4.8% for men, compared to 39.5% for women and 24.1% for men in our sample. Our data support previous findings that this population does undertake annual GP visits at which STI screening and testing might be opportunistically offered. Women, in particular, discussed sexual health with their GPs, likely during consultations for contraception. It would appear that, like other studies of chlamydia testing in general practice, GPs providing care to these students are not taking full advantage of opportunistic chances for chlamydia testing for this age group (Lorch et al., 2013). Significant work is being conducted in this regard with the ACCEPt (Australian Chlamydia Control Effectiveness Pilot trial) assessing the impact of providing GPs with training and regular feedback about chlamydia testing (Lorch et al., 2013). Preliminary results indicate that GPs feel the intervention is effective in increasing their offers of chlamydia testing (Yeung et al., 2015) and that practice nurses might also be recruited to provide this service to young people if organisational barriers could be overcome (Lorch et al., 2015). Given the objectives of the latest National Sexually Transmissible Infections Strategy, research is currently underway to improve detection and treatment of chlamydia in young people aged 16 to 29 years of age (Hocking et al., 2015). Currently, almost 20% of chlamydia testing of young women aged 18-30 years occurs opportunistically at a Pap smear appointment. Changes to the Australian National Cervical Screening Program increasing the age of first recommended Pap smear from 18 to 25 years, might significantly impact young women’s chlamydia testing opportunities (Moreira et al., 2015).
In general there appeared to be positive attitudes towards sexual health checks, but participants appeared to need assistance with scheduling STI testing. In particular participants in this study would welcome reminders about STI testing either via email or text message. A systematic review and meta-analysis of randomised control trials evaluating the impact of text messages on uptake of clinic appointments has shown an increased odds ratio of 1.48 (95% CI: 1.33-1.72) over relatively short periods of time of up to 72 hours prior to already scheduled appointments (Rebecca Guy et al., 2012). In Australia, text message reminders have been successfully used to increase re-testing after chlamydia infection (R. Guy et al., 2013) and qualitative research has shown that text messages are an acceptable method for providing health related information and reminders for young Australians. In particular, a study with young Victorians found that young people found text messages particularly useful when they were engaging, positive, relevant and different: text messages with these characteristics reduced young peoples’ trepidation about STI testing (Gold, Lim, Hellard, Hocking, & Keogh, 2010). These initiatives might be used in combination with GP-focused interventions currently being trialed in Australia. (Walker et al., 2010) Despite a universal national medical insurance scheme which covers the majority of patient costs for GP visits, screening and treatment; students in this study still felt that cost was a barrier to more regular STI screening. Given that more than 80% of Australians over 15 years visit their GP annually (Duckett & Willcox, 2015) this provides further incentive to integrate STI screening into regular visits, thereby limiting additional costs to the patient.
The finding that participants in de facto relationships report the highest prevalence of STI testing in the past 12 months is puzzling. We speculate that this may be a reflection of the life stage of these students; perhaps moving to a university town (which we appreciate is not necessarily the case for the on-line students in our sample) results in new couples living together (and therefore reporting as de facto) sooner than might otherwise have been the case. Partners in these relatively new relationships might have done away with condom use to signify transition in their relationship (Macaluso, Demand, Artz, & Hook, 2000), but still be relatively unsure of sexual history. The impact of cohabitation, in the context of moving to another town to engage in study, and/or living in residential on-campus accommodation, on sexual health indicators and outcomes is potentially an area for further research. Equally, distance students might be undergoing similar transitions, although not in the university town.
Limitations
The sample frame for this study was not the complete student population and we had a relatively low response rate. That said, demographics for participants were reflective of “new to this university” 2012 enrolment demographics for 17 to 29 year olds in terms of gender (1:2 male to female ratio) and representation of indigenous students (3.3% within the sample and 3.9% enrolment). Females were more likely than males to participate in this survey but the higher representation of females may not be generalisable to all Australian university students. Similarly, evidence from research with Australian university students aged 17-19 years suggests that generalisations to non-university students from these type of data might be inappropriate (de Visser, Smith, & Richters, 2005). The study was conducted at a regional university and might therefore have limited generalisability to metropolitan areas. That said, nearly two thirds of the sample were not living on campus but numbers of students studying on-campus or online were comparable. Yet, given the cross-sectional nature of the data collected, we cannot be confident that differences in knowledge are directly attributable to the intervention mentioned earlier.
Conclusions
This study of sexual health among a population of students studying at a regional university confirms findings from previous research in Australia. Despite relatively high levels of knowledge, students’ condom use is not consistent and there is worrying evidence that condom use is least prevalent among those with the greatest number of recent sexual partners. Students in this study had generally positive attitudes towards condoms, but responses suggest that they would prefer their sexual partner(s) to broach condom use.
Recommendations for student services
Although students in this study were more likely to report having screened for STIs in the past 12 months than previous Australian studies of the general population, they still perceived barriers to accessing services. In particular, students wanted additional assistance in remembering to screen and with overcoming financial barriers to GP visits. Initiatives currently underway to address the high rates of STIs in Australia, chlamydia in particular, are focused particularly on making STI screening routine in already scheduled GP visits. This strategy will address the perceived needs of students in this study. Recommendations for student services from this study include:
-
Working closely with health services / medical practices to promote routine STI screening
-
Promotion of services that offer bulk-billed or free sexual health screens and/or provision of routine on-campus or accessible STI screening clinics
-
Use of email and/or SMS annual STI check reminders to students
-
Student education re: availability / access to condoms; the promotion of positive messages and attitudes towards condom use; education about the when, how and why of initiating or instigating conversations with sexual partners about protected sex (i.e. promote intentionality in all sexual partners re: condom/oral dam use irrespective of gender)
-
Education around the increased risk of both HIV and cancer from STIs
The authors may be contacted via
Catherine MacPhail
References
Department of Health. (2014). Third National Sexually Transmissable Infections Strategy 2014-2017. Canberra, ACT: Australian Government.
de Visser, R., & Smith, A. (2001). Relationship between sexual partners influences rates and correlates of condom use. AIDS Education and Prevention, 13(5), 413-427.
de Visser, R., Smith, A., & Richters, J. (2005). Can we generalise to other young people from studies of sexual risk behaviour among university students? Aust N Z J Public Health, 29(5), 436-441. doi: 10.1111/j.1467-842X.2005.tb00223.x
Duckett, S., & Willcox, S. (2015). The Australian Health Care System. Melbourne, Australia: Oxford University Press.
Flood, M. (2003). Lust, trust and latex: Why young heterosexual men do not use condoms. Culture, Health & Sexuality, 5(4), 353-369. doi: 10.1080/1369105011000028273
Garrett, C., Hocking, J., Chen, M., Fairley, C., & Kirkman, M. (2011). Young people’s views on the potential use of telemedicine consultations for sexual health: results of a national survey. BMC Infectious Diseases, 11(1), 285-295.
Gold, J., Lim, M. S. C., Hellard, M. E., Hocking, J. S., & Keogh, L. (2010). What’s in a message? Delivering sexual health promotion to young people in Australia via text messaging. BMC Public Health, 10, 792-802. doi: 10.1186/1471-2458-10-792
Guy, R., Hocking, J., Wand, H., Stott, S., Ali, H., & Kaldor, J. (2012). How Effective Are Short Message Service Reminders at Increasing Clinic Attendance? A Meta-Analysis and Systematic Review. Health Services Research, 47(2), 614-632. doi: 10.1111/j.1475-6773.2011.01342.x
Guy, R., Wand, H., Knight, V., Kenigsberg, A., Read, P., & McNulty, A. (2013). SMS reminders improve re-screening in women and heterosexual men with chlamydia infection at Sydney Sexual Health Centre: a before-and-after study. Sexually Transmitted Infections, 89, 11-15. doi: 10.1136/sextrans-2011-050370
Hocking, J., Temple-Smith, M., Poznanski, S., Guy, R., Low, N., Donovan, B., . . . Fairley, C. (2015). Australian chlamydia control effectiveness pilot: preliminary results from a trial of chlamydia testing in general practice. Paper presented at the STI & HIV World Congress, Brisbane, Australia.
Hoff, T., Green, L., & Davis, J. (2003). National Survey of Adolescents and Young Adults: Sexual Health Knowledge, Attitudes, and Experiences. Pub. No. 3218. Menlo Park, CA: Henry J. Kaiser Family Foundation. http://www.kff.org/youthhivstds/upload/National-Survey-of-Adolsecents-and-Young-Adults.pdf
Kang, M., Skinner, R., & Usherwood, T. (2010). Interventions for young people in Australia to reduce HIV and sexually transmissible infections: a systematic review. Sexual Health, 7(2), 107-128.
Kong, F., Hocking, J., Merritt, T., Pirotta, M., Heal, C., Bergeri, I., . . . Hellard, M. (2011). Australian general practitioner chlamydia testing rates among young people. Medical Journal of Australia, 194(5), 249-252.
Lorch, R., Guy, R., Temple-Smith, M., Vaisey, A., Wood, A., Ford, B., . . . ACCEPt Consortium. (2015). The impact of education on Australian practice nurses’ knowledge and attitudes in relation to chlamydia testing: findings from the Australian Chlamydia Control Effectiveness Pilot (ACCEPt). Paper presented at the STI & HIV World Congress, Brisbane, Australia.
Lorch, R., Hocking, J., Temple-Smith, M., Law, M., Yeung, A., Wood, A., . . . Guy, R. (2013). The chlamydia knowledge, awareness and testing practices of Australian general practitioners and practice nurses: survey findings from the Australian Chlamydia Control Effectiveness Pilot (ACCEPt). BMC Family Practice, 14, 169.
Macaluso, M., Demand, M. J., Artz, L. M., & Hook, E. W. I. (2000). Partner type and condom use. AIDS, 14(5), 537-546.
Moreira, C., Van Gemert, C., Hocking, J., Lim, M., Bateson, D., McNamee, K., . . . El-Hayek, C. (2015). Screening for chlamydia concurrently with a routine pap test in primary care: could cervical screening changes impact on chlanydia testing? Paper presented at the STI & HIV World Congress, Brisbane, Australia.
Roberts, L. (2014, 8 August). Grim record for sex bug, The Armidale Express.
Senior, K., Helmer, J., Chenhall, R., & Burbank, V. (2014). 'Young clean and safe?'Young people’s perceptions of risk from sexually transmitted infections in regional, rural and remote Australia. Culture, Health & Sexuality, 16(4), 453-466.
Smith A, Agius P, Mitchell A, Barrett C, Pitts M. 2009. Secondary Students and Sexual Health 2008, Monograph Series No. 70. Melbourne: Australian Research Centre in Sex, Health & Society, La Trobe University.
The Kirby Institute. (2015). HIV,viral hepatitis and sexually transmissable infections in Australia Annual Surveillance Report 2015. In U. The Kirby Institute (Ed.). Sydney, NSW.
Tsouros, A., Dowding, G., Thompson, J., & Dooris, M. (Eds.). (1998). Health Promoting Universities: Concept, experience and framework for action. Copenhagen: World Health Organization Regional Office for Europe.
Walker, J., Fairley, C. K., Walker, S. M., Gurrin, L. C., Gunn, J. M., Pirotta, M. V., . . . Hocking, J. S. (2010). Computer Reminders for Chlamydia Screening in General Practice: A Randomized Controlled Trial. Sexually Transmitted Diseases, 37(7), 445-450. doi: 10.1097/OLQ.0b013e3181cfcb4c
Yeung, A., Hocking, J., Vaisey, A., Lorch, R., Guy, R., Fairley, C., . . . ACCEPt Consortium. (2015). “It opened my eyes” - examining the impact of the Australian Chlamydia Control Effectiveness Pilot (ACCEPt) on chlamydia testing practices of general practitioners. Paper presented at the STI & HIV World Congress, Brisbane, Australia.
Gina brought her statistical expertise to this project which could not have been completed without her. Gina was awarded her PhD at UNE in 2015 and she received the VC Doctoral Research Medal that same year. Her PhD research investigated intimate partner violence experienced by young Australian women and its mental health consequences, comparing metropolitan, regional and remote areas of Australia.